Deep Vein Thrombosis (DVT) – VTE , PE
Venous Thromboembolism (VTE) is an umbrella term that includes two conditions: Deep vein thrombosis (DVT) and pulmonary embolism (PE). DVT is a blood clot that forms in a vein deep in your body. … Read More
Top Doctors For Deep Vein Thrombosis (DVT) – VTE , PE Treatments





Top Hospitals For Deep Vein Thrombosis (DVT) – VTE , PE Treatments



































Deep Vein Thrombosis (DVT) – VTE , PE
Venous Thromboembolism (VTE) is an umbrella term that includes two conditions: Deep vein thrombosis (DVT) and pulmonary embolism (PE).
What do you mean by Deep Vein Thrombosis (DVT)?
Deep Vein Thrombosis is a medical condition in which a blood clot forms within the deep vein. DVT most commonly occurs in the lower leg or thigh region. However, in a few cases, it can occur in other parts of the body. DVT is considered a medical emergency that has to be treated on an emergency basis. If left untreated, it can be fatal [1].
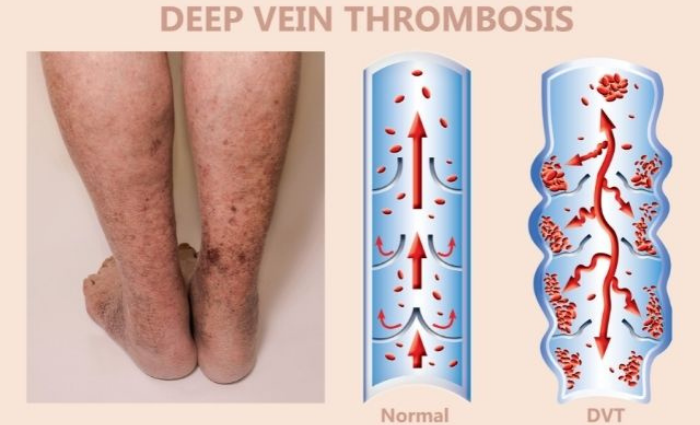
Deep vein thrombosis (DVT) is a condition that occurs by the formation of blood clots in the deep veins. The latter include large veins, anatomically located under the deep fascia. It is a common disease that most commonly affects the leg veins and pelvis and can lead to pulmonary embolism (PE). DVT and PE are related, so they are often called venous thromboembolism (VTE).

Causes
What are the most common causes associated with DVT?
-
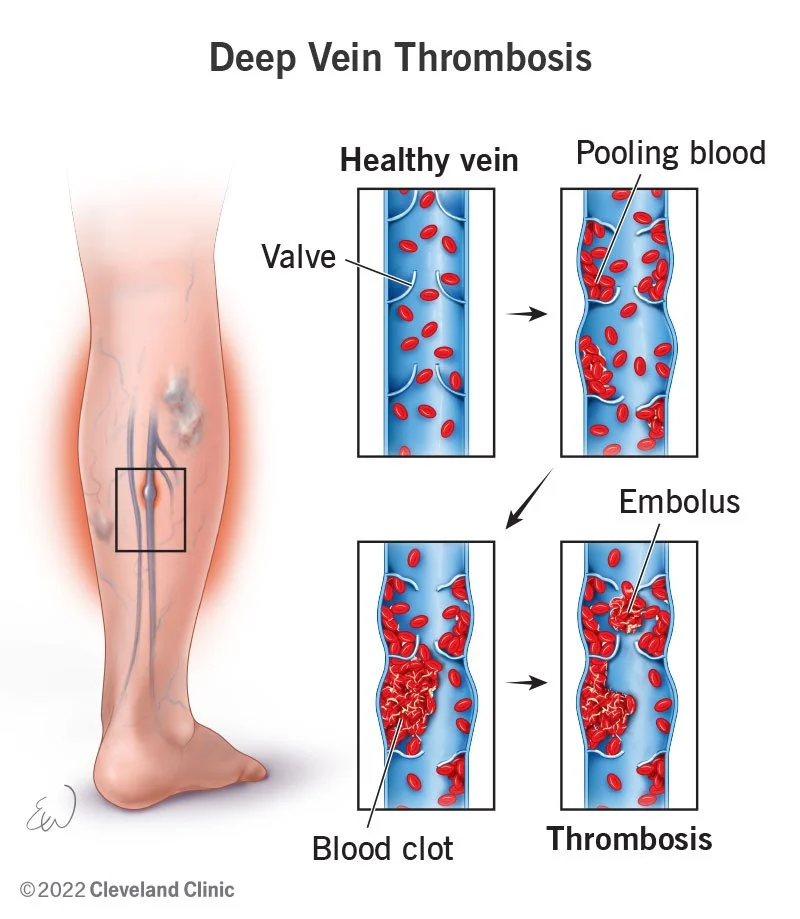
- German physician Rudolf Virchow described three factors contributing to the development of deep vein thrombosis: stasis (a significant slowdown in blood flow), vascular damage, and hypercoagulation (increased blood clotting).
- In addition to postoperative and trauma-related causes, stasis plays the primary role in causing deep vein thrombosis.
- DVT more often begins at the venous valves due to low blood flow
- Antithrombotic proteins such as thrombomodulin and endothelial protein C receptor are synthesized locally on valves and are sensitive to hypoxia (lack of oxygen) and inflammation. Due to the lack of oxygen, the concentration of procoagulants, such as tissue factor on the endothelium and P-selectin (an adhesion molecule), can increase. Further, it increases blood coagulation, thereby creating conditions for developing thrombosis.
- An increased risk of blood clots is associated with high clotting factors, namely factor VIII, von Willebrand factor, factor VII and prothrombin. An increase in their level is observed with the reduced effectiveness of natural anticoagulants (substances that reduce blood clotting). At the same time, the likelihood of immobilization and infection becomes higher.
DVT can occur for several reasons, including damage to a vein, such as a fracture or surgery, or slow blood flow, such as lying in bed or sitting for long periods like a long flight. Other risk factors include:
-
- Being pregnant
- The use of hormone replacement for menopause or birth control pills
- Being overweight
- Having cancer
- An inherited condition can increase your likelihood of forming clots or decrease your ability to dissolve them.
Symptoms
What are the symptoms associated with DVT?
-
- The primary symptom of deep vein thrombosis is lower extremity edema in most cases. The severity of the lesion will depend on its extent.
- In the case of iliofemoral thrombosis (the formation of blood clots in the deep veins at the thigh and pelvic region), the entire lower limb is swelling, possibly with the genitals unilateral edema and significant pain syndrome.
- Change in color of the limb. Motor activity decreases due to severe edema or pain syndrome.
- DVT typically begins below the level of the lower leg and popliteal veins. Most thrombi form in the deep veins below the trifurcation (a division of the artery into three smaller branches) of the popliteal artery (distal DVT).
- Thromboembolic symptoms such as new or worsening dyspnea, chest pain, or persistent hypotension (low blood pressure) with no alternative cause occur in about 30–40% of patients with VTE.
- The most severe form of venous thrombosis is when the auxiliary outflow pathways are blocked, called “blue phlegm”. The limb becomes blue in color, wood density, puffiness appears, movements, and sensitivity of the limb is reduced or absent.
- The symptoms of thrombosis of the inferior vena cava are edema and cyanosis (blue color) of the lower half of the trunk, lower extremities, and genitals.
- In floating (floating) or parietal thrombi cases, clinical symptoms may correspond to the involvement of the femoral or iliac veins.
DVT symptoms, usually limited to one leg at a given time, include:
-
- Swelling of the leg
- Pain or tenderness in the leg, often similar to the symptoms of a muscle cramp (or injury) that does not resolve
- Increased warmth in the area
- Red or discolored skin
Patients suffering from upper extremity DVT may experience symptoms such as:
-
- Neck pain
- Shoulder pain
- Swelling in the arms and hand
- Change in color of the skin
- Weakness in the affected area
- Pain that moves from arm to forearm.
How do we diagnose Deep Vein Thrombosis?
The diagnosis of DVT requires some special tests to be performed by the doctor while doing a physical examination of the patient. A few of the tests are listed below:
-
- Homans’ symptom- Pain in the calf muscles during dorsiflexion of the foot.
- Moses’ symptom- Pain when the lower leg is squeezed in the anteroposterior direction.
- Loewenberg’s symptom – Pain in the calf muscles at a pressure of up to 80 mm Hg. by the cuff of a sphygmomanometer (a device for measuring blood pressure).
- Recognizing symptoms is critical for the early diagnosis of DVT. The first step is to assess the risk of thromboembolism. Several systems have been developed, for example, the Wells or Geneva scale. They are a list of features, each corresponding to a certain number of points. For example, according to the Wells scale, the statement “Previously suffered PE or deep vein thrombosis” corresponds to 1.5 points. If the indicator is less than two points, the probability of PE is considered low, and if the value is more than six points, it is considered high. According to the Wells scale, with a low, moderate, and high probability of PE, the incidence of this disease is about 6, 23, and 49%, respectively.
- The Geneva scale also evaluates thromboembolism according to several parameters, including age, pulse rate, hemoptysis, etc.
- Wells’s criteria are also widely used to assess the likelihood of deep vein thrombosis. Wells’s criteria include limb edema, local tenderness, and cancer diagnosis. D-dimer testing is often done for patients with suspected low to moderate DVT levels. A normal D-dimer in low-to-moderate-risk patients allows DVT to be ruled out confidently. Duplex ultrasonography is indicated if the D-dimer is abnormal at any level of risk. All high-risk patients should receive a diagnostic ultrasound (ultrasound) scan and a D-dimer test. A positive ultrasound for DVT suggests active treatment, whereas a negative ultrasound in a high-risk patient requires a repeat ultrasound within seven days.
- Venogram- During this test, a dye is injected into the vein, followed by an X-ray taken in the area where the doctor suspects DVT [2].
- Magnetic Resonance Imaging (MRI)- MRI scan is done to diagnose DVT in veins of the abdomen.
How can DVT be cured?
Deep Vein Thrombosis Treatment
-
- The role of an inferior vena cava filter in treating deep vein thrombosis is uncertain. Filter insertion, according to guidelines, is possible within the first four weeks only if there are contraindications to anticoagulant therapy, including active bleeding or recent major surgery. Anticoagulant therapy continues to be the mainstay for IVC thrombosis. It is carried out to prevent further clot formation and growth and facilitate the natural mechanisms of clot lysis (dissolution).
- Multiple adjunctive therapies in the acute process may be effective in the correct clinical setting, including systemic fibrinolytic therapy, catheter-directed thrombolysis, pharmacomechanical thrombectomy, aspiration thrombectomy, surgical thrombectomy, and stenting.
- Systemic thrombolytic therapy has shown significant short-term benefits over anticoagulant therapy, including complete clot lysis by 45% versus 5% and partial lysis by 65% versus 20%, and a significant reduction in the incidence of post-thrombotic syndrome. These benefits are unfortunately accompanied by a high risk of severe bleeding, including intracranial hemorrhage (14% with thrombolytic therapy versus 4% with heparin)
- DVT requires a dynamic ultrasound to evaluate anticoagulant therapy with an assessment of both limbs to exclude simultaneous (combined) thrombosis.
- Blood thinners: These drugs are also called anticoagulants, most commonly used to treat DVT. These drugs help in preventing the formation of new clots in the bloodstream. A few anticoagulant drugs are – heparin, warfarin, low molecular weight heparin, edoxaban, apixaban, rivaroxaban, etc.
- Compression stockings: These are the special knee stockings that help prevent swelling associated with DVT.
The treatment regimen for DVT depends on the severity of the condition and the person’s general health. Iliofemoral thrombosis leads to the development of a post-thrombotic disease, accompanied by the development of chronic limb edema and hyperpigmentation. However, with early detection of thrombosis and adequate therapy, clinical symptoms may be minimal.
FAQ
How rare is Deep Vein Thrombosis (DVT)?
According to studies conducted in the United States, among the country’s population, DVT develops annually in 375,000-425,000 patients, and a significant number of cases of the disease end in the death of patients. Every year, deep vein thrombosis and pulmonary embolism occur in 1-2 people out of 1000. It occurs:-
-
- 1: 100,000 children
- 1:10 000 at reproductive age
- 1: 1000 in later middle age
- 1: 100 in old age
What are the risk factors of developing Deep Vein Thrombosis (DVT)?
The following are common risk factors that can lead to the development of DVT:
-
- prolonged hospitalization
- the presence of an active oncological condition
- major surgery
- decompensated diseases
- Natural anticoagulant deficiencies, antithrombin and anticoagulant S, as well as protein C, protein S, and anticoagulant C.
- Many drugs, including oral contraceptives and female hormones, increase the risk of developing thrombosis. Combined oral contraceptives containing estrogen and progesterone increase the risk of venous thrombosis by 2-4 times.
- Obesity is another risk factor that almost doubles the chance of blood clots.
- Genetically associated (hereditary).
How to prevent DVT?
Appropriate use of DVT prophylaxis in inpatients is essential to reduce the risk of post-thrombotic complications and fatal and non-fatal pulmonary embolism. Methods for preventing DVT include:
-
- Aspirin use (the role of aspirin in preventing DVT is still controversial).
- mechanical prevention using graduated (uneven pressure) compression and intermittent pneumatic compression stockings
What are the most common complications of Deep Vein Thrombosis?
Postthrombotic syndrome (PTS) is a chronic, long-lasting proximal deep vessel thrombosis outcome. This is a clinically chronic process. 20 to 50% of patients with proximal DVT will suffer from post-thrombotic syndrome within two years. PTS may be due to incomplete vessel patency restoration or damage to the venous valves. This causes valve reflux (i.e., reverse blood flow). Clinically, PTS manifests as heavy legs, fatigue, pain, swelling, and soreness in the legs. Severe PTS, found in 3% of patients after DVT, is additionally accompanied by venous ulcers.
References
- https://www.cdc.gov/ncbddd/dvt/facts.htmlhttps://www.healthline.com/health/deep-venous-thrombosis#diagnosis
