Guillain barre syndrome (GBS) is a rare autoimmune disorder in which the immune system attacks the nerve cells of the peripheral nervous system ( it is a network of cells found outside the brain and spinal cord, these cells connect the brain and rest of the body and aid in transmitting the signals to the […] Read More
Guillain barre syndrome (GBS) is a rare autoimmune disorder in which the immune system attacks the nerve cells of the peripheral nervous system ( it is a network of cells found outside the brain and spinal cord, these cells connect the brain and rest of the body and aid in transmitting the signals to the body muscles). It was named after the French Neurologists Georges Guillain and Jean Alexandre Barre and French physician Andre Strohl in 1916[1]. Damage to the peripheral nervous system results in weakness, numbness, and tingling sensation, and in severe cases, the patient finds difficulty in breathing and paralysis of the whole body.
According to the National Institute of Neurological Disorders and Stroke, Guillain barre syndrome is estimated to affect 1 in every 100,000 Americans per year. The incidence rate is higher in men than women (1.5:1 ratio). GBS affects all age groups; however, the occurrence is higher in middle-aged and old age groups (50-70yrs).
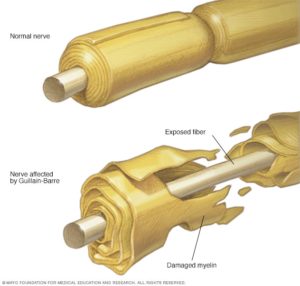
Pic Courtesy: MayoclinicTYPES OF GUILLAIN BARRE SYNDROME:They include:
It is most commonly found in North America and Europe. 40% of the patients are usually affected by C.jejuni. It is characterized by muscle weakness which begins at the lower part of the body and later affects the upper part of the body. It affects the myelin coating affecting nerve signal transmission. Symptoms generally resolve with remyelination [2].
Miller Fisher Syndrome (MFS)
Here, paralysis occurs in the eyes. It is mainly associated with unsteady gait(movement). It is most common in Asia and less common in the USA. It affects the cranial nerve causing abnormal muscle coordination resulting in clumsy gait, weakness of the eye muscles, and absence of tendon reflexes. Recovery generally occurs in one to three months.
Acute Motor Axonal Neuropathy (AMAN) and Acute Motor Sensory Axonal Neuropathy (AMSAN)
They are rarely found in the US but quite common in Japan, China, Mexico, etc. The axons are damaged by the autoimmune response of the immune system. AMAN is a motor disorder characterized by rapidly progressive symmetrical weakness and respiratory failure. It is more prevalent in the pediatric age group. Marked muscle wasting is the most characteristic feature of AMSAN. The prognosis of AMSAN is poorer when compared to AMAN.
Acute panautonomic neuropathy
It is the rarest form of GBS, involving both sympathetic and parasympathetic nervous systems. Patients usually have bladder and bowel retention, postural hypotension, pupillary abnormality, decreased salivation, and lacrimation. Recovery is generally time taking and do not recover completely.RISK FACTORS
Age; although it affects all ages, its risk increases as you get older.
Rarely influenza vaccinations or childhood vaccinations [3].
Campylobacter is found in undercooked poultry.
DIAGNOSIS OF GUILLAIN BARRE SYNDROME
Since symptoms are similar to other neurological disorders or conditions such as botulism, meningitis, or heavy metal poisoning, which could be caused by lead, mercury, and arsenic, it is challenging to diagnose Guillain-Barre syndrome at first.
However, when suspicious symptoms arise, the following diagnostic test can be used:1. Spinal Tap/ Lumbar PunctureThis procedure involves puncturing the lower back to take a small amount of fluid from the spine, then testing to check protein level. This fluid is called cerebrospinal fluid. In Guillain-Barre syndrome, the cerebrospinal fluid’s protein level is higher(>0.55g/dl) than the normal CSF. This is usually done 10days after the onset of symptoms. 2. Electromyography (EMG) and Nerve Conduction Study (NCS)This is a nerve function test. It works using electrical activity from the muscle to check muscle weakness caused by nerve damage or muscle damage.
EMG might be typical in the case of acute nerve lesion; abnormalities might be noticed after 3-4 weeks.
Abnormalities in NCS represent specific findings for classic GBS. You will be checked for recent viral infection absent or diminished deep tendon reflexes in weak limbs.
3. Peripheral Neuropathy workup 4. Serological Studies: Limited value in the diagnosis of GBS5. Serum Autoantibodies: Specific autoantibodies found in GBS are Anti GM1 antibodies Anti GQ1b antibodies.6. MRI imaging7. Muscle Biopsy and Histology.GUILLAIN BARRE SYNDROME TREATMENTCurrently, Plasmapheresis and intravenous immunoglobulins are the two primary immunotherapy for GBS treatment. The treatment is made to reduce the severity of the immune attack and improve body function such as lung function while helping the nervous system recover. This treatment includes: 1. Plasma Exchange (also called Plasmapheresis). In Guillain barre Syndrome, the immune system produces antibodies that attack the nerves of the nervous system, mistaking them as harmful foreign substances to the body. Plasmapheresis aims to remove such antibodies, immune complexes, and cytotoxic substances produced from the blood. This process involves the removal of blood from your body by a machine that removes the antibodies from the blood and then returns the blood to your body. This process usually takes over 10days, and recovery is good. 2. Intravenous Immunoglobulin (IVIG)This is the most common and safer technique used in treating GBS. This is the most preferred method in hemodynamically unstable patients. Immunoglobulin contains normal healthy donor antibodies. On administration of high-dose immunoglobulins helps in blocking antibodies causing GBS. 3. Immune Adsorption: it is an alternative technique used in treating GBS, which is still under the early stages of investigations [4].4. Analgesics: Medications such as NSAIDs or acetaminophen are usually recommended for pain relief management… 5. Prevent thromboembolism: LMWH (low molecular weight heparin) is administered to prevent DVT and embolism.6. Physical and occupational therapy will be carried out. This involves the manual movement of your arms and legs. Primarily done in severe cases.7. ICU care: Good supportive care is critical in treating GBS. Intensive care includes respiratory therapy, cardiac care, nutritional support, closely monitoring for infectious complications (e.g., septicemia, UTI, pneumonia, etc.).COMPLICATIONSThe complications involved with Guillain barre syndrome include:
Difficulty with breathing; The muscles that help to breathe may become weak or paralyzed. Approximately 22% of people with Guillain-barre syndrome will need aid from a machine(ventilator), so they can breathe, especially within the first week of treatment.
Residual weakness or numbness.
Heart and blood pressure fluctuations are common complications of Guillain-barre syndrome. Cardiac arrhythmias and BP fluctuations are the most common side effects of GBS.
Pains; Severe nerve pain may be experienced even after recovery.
Development of blood clot, which is due to immobility. Blood thinners will be advised.
Development of pressure sores.
Sluggish bowel and bladder functions.
GUILLAIN BARRE SYNDROME PROGNOSIS Approximately 2-5% of people with Guillain barre syndrome experience a relapse. It has a high recovery rate even in severe cases and a Mortality rate of 4% to 7%. However, few deaths have been recorded from complications such as respiratory distress syndrome.
Symptoms
GUILLAIN BARRE SYNDROME SYMPTOMS
Symptoms are usually progressive and they include:
Tingling sensation in the toes and legs
Muscle weakness in the legs that travels to the upper body with time.
Difficulty when walking
Difficulty when moving your eyes or face
Double vision
Difficulty in talking, chewing, and swallowing
Severe lower back pain which gets worse at night
Difficulty with bladder control
Increase in heart rate
Difficulty in breathing
Paralysis
Causes
GUILLAIN BARRE SYNDROME CAUSES
The cause of Guillain barre syndrome is unknown, but most cases report incidents of infection such as respiratory or gastrointestinal infection.
According to reports, two-third of people with Guillain barre begins soon after they had been sick with diarrhea or a lung infection which implies that it could be triggered by an improper immune response to a previous illness.
The incidence of developing Guillain barre is higher after the flu or an infection such as COVID-19.
FAQ
How long does Guillain Barre last?
Guillain barre syndrome tends to worsen within two weeks after its onset but gets worst after 4weeks without treatment. However, recovery may take 12months or three years when appropriately treated, depending on how severe the condition was.
Can Guillain barre syndrome affect the brain?
Guillain barre syndrome affects the peripheral nervous system. The peripheral nervous system consists of nerve cells except the brain and spinal cord.
Does Guillain barre show on MRI?
Although not frequently used, it shows affected areas of the peripheral nervous system as thickened and marked enhancement.
Can Guillain syndrome cause neuropathy?
Since Guillain barre syndrome is an autoimmune disorder, it is possible for neuropathy to occur as the axon in the motor nerve is affected.
What triggers Guillain syndrome?
Guillain barre syndrome could be triggered by viral infections, surgery, gastrointestinal infections, or lung infections. In rare cases, vaccinations.
Please feel free to reach out if you have any questions about medical tourism, air ambulance or surrogacy services. We will quickly get back with an answer or solution – looking forward to hearing from you!