Nephroblastoma (Wilms Tumor)
Nephroblastoma, which is also known as Wilms’ tumor is a type of rare kidney cancer that often occurs in children. This type of kidney cancer is also the fourth very most common type of childhood cancer and roughly around 500 children in the world are newly diagnosed with the situation each year. Mostly, Wilms’ tumor is typically diagnosed in kids around 3 years of age. This rare kidney cancer can sometimes occur in older children and adults too.
Read MoreTop Doctors For Nephroblastoma (Wilms Tumor) Treatments
















































Top Hospitals For Nephroblastoma (Wilms Tumor) Treatments










































Nephroblastoma (Wilms Tumor)
Table of contents
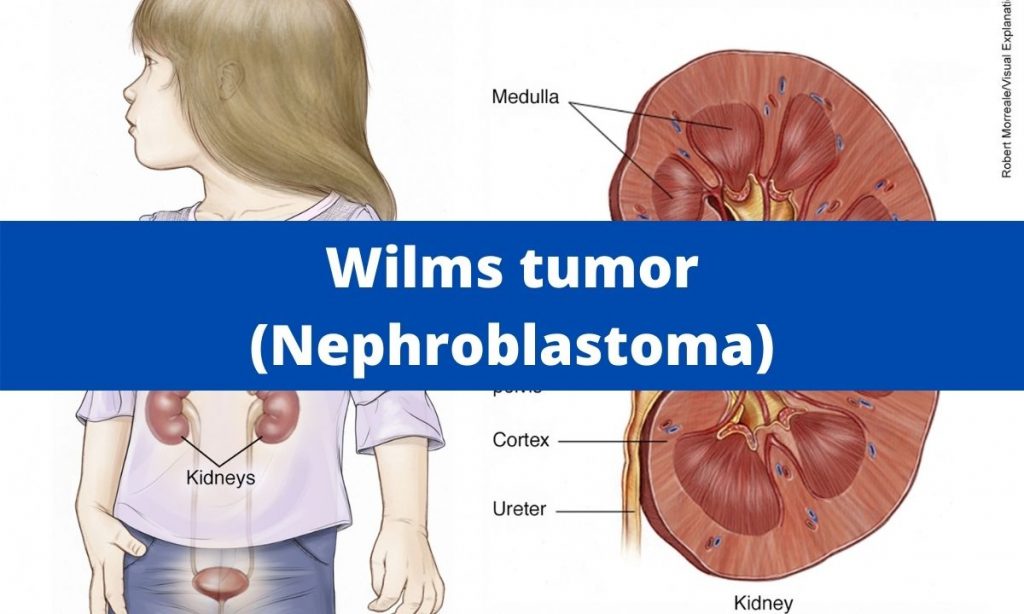
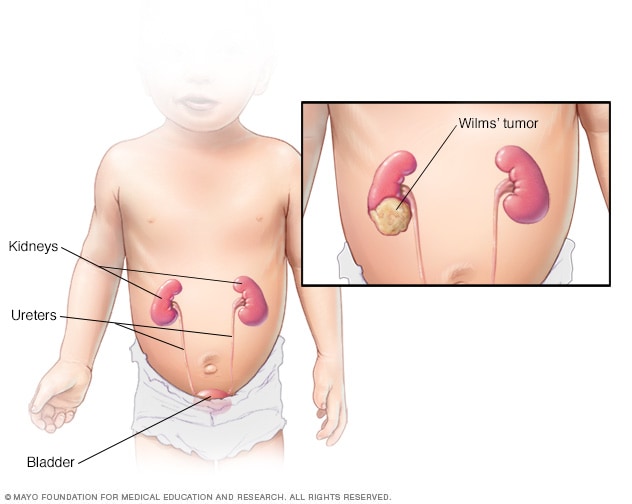
What are Wilm’s tumors?
Wilm’s tumor, also known as Nephroblastoma, is a rare kidney cancer that primarily affects children. It is the most common malignant cancer of the kidney in children. It most commonly affects children from 2-5years of age. Wilm’s tumor most commonly affects one kidney. However, in a few cases, it can affect both kidneys.
What are the types of Wilm’s tumors?
Wilm’s tumors are classified into two major types based on histological findings. They are:
- Unfavorable (anaplastic) Histology: This type of tumor has a nucleus in the cells and often looks very large and distorted in unfavorable histology. This type of tumor is often referred to as Anaplasia. These tumors are difficult to treat since they can spread to other organs easily.
- Favorable Histology: This type of tumor doesn’t have Anaplasia. Most tumors are easier to cure since over 90 percent of Wilms’ tumors have favorable histology. The outcome of these tumors is good.
How is Wilm’s tumor diagnosed?
The doctor will advise the patient to undergo a couple of blood tests and other investigations to diagnose Wilm’s tumor. A few of them are listed below:
- Physical examination- The doctor will record the patient’s complete medical and family history. The doctor will examine the patient thoroughly.
- Blood and Urine tests- These tests are done to evaluate the function of the kidney.
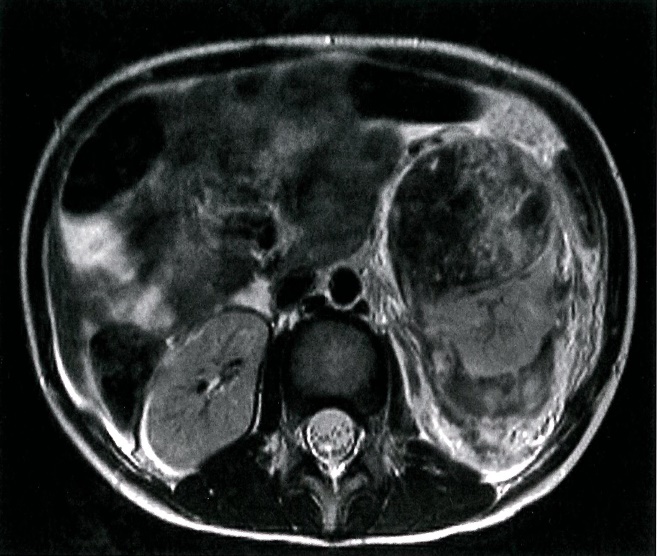
- Imaging tests- They include CT-scan, X-rays, MRI scans, PET-scan, and renal ultrasonography. These tests help in finding the location of the tumor and the size of the tumor.
- Biopsy- During this procedure, a small tumor sample is taken out and sent for histological evaluation. However, this procedure is not carried out routinely for Nephroblastoma. It is advised only in case of atypical tumors.
How is Wilm’s tumor treated?
The treatment procedures for Nephroblastoma are listed below:
- Surgery
- Radiation Therapy
- Chemotherapy
Most of the time, children undergo a combination of treatments. However, surgery is generally the first treatment that doctors advise the patient, with the main goal of the surgery being to remove the tumor.

Surgery for Wilm’s tumor includes:
- Removing part of the kidney affected
- Removing the affected kidney and surrounding tissue
- Removing all or part of both kidneys.
If the surgery isn’t successful, the child has to undergo chemotherapy or radiation therapy if the tumor isn’t removed successfully. Apart from that, medications and the extent of treatment will normally vary depending on the child’s condition.
Symptoms
Children between 2 to 4 diagnosed with Wilms’ tumor often show the following signs and symptoms.
- Constipation
- Swelling, discomfort, and pain in the abdomen
- Nausea and vomiting
- Weakness and fatigue
- Loss of appetite
- Fever
- Discoloration or blood in the urine
- High blood pressure
- Shortness of breath
Causes
Though researchers still have not found what causes Nephroblastoma or any clear links between the disease and environmental factors, these are a few factors that cause the Wilms’ tumor.
Genetic Factors:
Though children don’t directly inherit the condition from their parents, researchers believe certain factors might raise the chance of a child developing Wilms’ tumor genetically. These are the following genetic syndromes that increase the chances of a child being diagnosed with Nephroblastoma:
- WAGR syndrome includes Wilm’s tumor, aniridia, genital and urinary system abnormalities, and intellectual disabilities.
- Densys-Drash syndrome
- Bloom syndrome
- Perlman syndrome
- Sotos syndrome
- Edward’s syndrome (Also called Trisomy 18)
- Frasier syndrome
- Beckwith – Wiedemann syndrome
Frasier, WAGR, and Denys-Drash syndrome are linked to mutations in the WT1 gene. On the other hand, Beckwith-Wiedemann syndrome is linked to mutations in the WT2 gene. All these genes are found in chromosome 11. And changes in these genes account for a small percentage of Nephroblastoma in children below 3 years of age. Apart from that, children with certain birth defects are also more likely to develop Nephroblastoma. These are the following birth defects that are associated with the condition.
- Aniridia
- Hemihypertrophy
- Cryptorchidism
- Hypospadias
FAQ
The five-year survival rate of a kid with Nephroblastoma is 81%.
Unlike any cancer, the spreading of the disease to almost all organs is a serious complication. And some of the side effects of the treatment are as follows: Hair loss, fatigue, nausea, and vomiting.
Wilm’s tumor can’t be prevented. However, the various screening tools can always ensure early detection.
Nephroblastoma can mostly spread to lymph nodes in the abdomen and the lung (rarely to the liver). It does not spread to the bones, bone marrow, or brain.
Most of the time, relapses occur within two years of diagnosis of the original Nephroblastoma, yet for some children, it can come back later. And this is for 85% of cases.
The risk factors are listed below:
i. African-American race
ii. Family history of Wilm’s tumor.
iii. Gender- girls are most likely to have this tumor compared to men.
iv. Age- affects children between 3-5years.
v. Children with birth defects include- cryptorchidism, hypospadias, aniridia, and hemihypertrophy.
Picture Courtesy: Medindia
Wilm’s tumor has a very good prognosis. About 80-90% of the children diagnosed with Wilm’s tumor with favorable histology can be cured completely. However, the outcome is not good for patients with anaplastic histology. Therefore, patients who have undergone treatment should have a regular follow-up with the doctor and follow the doctor’s instructions strictly.